
Posted 1291 days ago
By Dr. Ahmad al-Hassiny
Sponsored by Ivoclar
In part II of this series of three parts, Dr. Ahmad al-Hassiny shares the work flow processes that maximize their clinical efficiency and profitability, as well as useful advice to guarantee the success of the restoration CAD/CAM of a single vision.
If you missed me
Part II
The transition from a traditional dental practice to a digital workflow sacrifices a unique set of challenges for professionals immersed in the conventional analog treatment process. Certainly, that was true in our situation here in Wellington, New Zealand, where our operated clinics would independently have to make that transition. As you could imagine, the first challenge was the expense of equipping each of our clinics with the CEEC® CAD/CAM systems, much less all other intraoral scanners, milling machines, 3D printers that we have bought at the years. This company was an important and important investment, not to mention the inventory of materials that each clinic would require. The second important obstacle, and probably the most critical challenge, was the learning curve for our associates and us. However, we are all that the expense would be justified and the profitable initiative if we could improve a digital workflow that was efficient, the maximized clinical processes and simplify effective enough to minimize the chair time for patients.
As we carry out our transition, digital technologies matured, as did the ground materials. Modern intraoral scanners are now much faster and more precise; More precise milling technologies; More intuitive and easy -to -use CAD software; And much stronger, more predictable and aesthetic materials. The most important thing is that our associates and I work very hard to dominate and rationalize our work flow processes, which directly impacted the profitability of our practices.
Today, our standard workflow from preparation to design and factory for a single crown can be achieved in 45 minutes or less, and the final crown is sitting in an hour at an hour and a half on average. After preparing the tooth, we routinely use the retraction cable (Figure 1) to move the gingiva and guarantee a precise scan of the margins and a dry operation field to avoid the pollution of the blood, the saliva or the Greek liquid. We take an intraoral scan using CEREC Priman for our dentistry and design of the same day using the biogeneneric cerec software. Our dental assistants are fully trained to be competent with the use of CAD software (Figure 2-3) and make all our CAD designs with clinical supervision, and the final design approach, and the design is then for the milling machine (Figure 4). Our staff is also trained in all the steps after processing, from the crystallization shooting process to the bite and the glazing of the final restoration (Figure 5). Measurement, the retraction cable remains in place so that the duration of the seat of the final crown, the adjustment in the margin is clearly visible and once cemented, the excess cement is removed as the cable is removed. The most critical for this process and the profitability of our practices is that while the design, grinding and subsequent processing occurs, our doctors are busy seeing and treating other courtyards. Single visit dentistry can be immensely profitable if it is done well. Now, 95 percent of the work that was sent to the laboratory is complete internal. This effectively reduced our laboratory bill by more than 70%.

Figure 1: Application of a retraction cable around a tooth prepared before scanning displaces the gingiva and guarantees a precise scan of the margins, as well as a dry operation field.

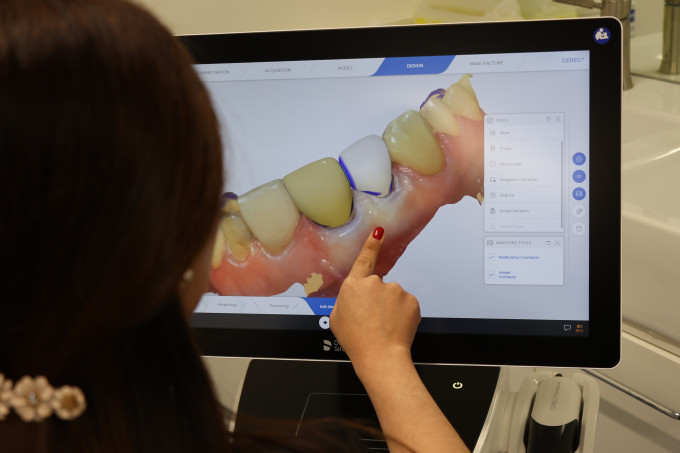
Figures 2-3: Our dental assistants are completely trained to be competent with CAD software and make all our CAD designs with clinical supervision, which frees me to see the duration of other patients this work flow process the same day.

Figure 4: Our dental assistants also process and grind restorations on the same day.

Figure 5: My dental assistants also perform posterior spots on the mill, glazing and crystallization of IPS crowns E.MAX CAD. The Programmat CS2 shooting oven allows IPS E.Max CAD crowns to be fired in 15 minutes.
My advice for colleagues who are thinking of entering this space is not to be afraid of cost, the learning curve and the new work flow processes. We hire new associates soaked in the analog process, and in approximately two months or less, they are competent with the CAD/CAM process and the workflow. Even if you are already doing dentistry on the same day, the key to that transition or perfect your workflow is to induce themselves in online learning and in person of those who have dominated the CAD/CAM teams and the digital workflow process.
In addition, choose a restorative material that offers the confidence of predictability, flexibility, strength and aesthetics in all areas of the mouth. Here in New Zealand, zirconia is not the typical reference material, as it is in the United States. We need a material that the research has shown to have all these characteristics, as well as a fracture rate of less than 1%-2%. That is why we choose IPS E.Max. Millions of these restorations have been placed in the leg worldly, and research on this material is extensive.
A vital key to success when using CAD/CAM processes is teeth preparation. Above all, this is more important. If it is low or prepared, the whole process will be more challenging, slower and less efficient. I, and many of my colleagues, think that we were teachers of teeth preparation until we went to CAD/cam and could see preparations on the computer screen. With the ability to examine all aspects of its 3D preparation, you can see any defect and make corrections while the patient is in the chair. The use of intraoral scanners makes it a better dentist due to the instantaneous comments it receives on the quality of its preparation.
A critical area that requires duration of attention to the preparation of the tooth for the CAD/CAM process is an adequate occlusal reduction. The main reason for the fault of totally ceramic restorations is the inadequate reduction of the tooth. Department of the restorative material used, it needs at least 1 mm or an occlusal reduction to guarantee the integrity and durability of that restoration. If it does not reduce the occlusal to that degree, the software will compensate and end with a poor restoration that invades a minimum thickness or a high point in the finished crown that runs the risk of fracture of the occlusal forces.
Without a doubt, the CAD/CAM process is extraordinarily precise and can be used for a wide range of single visit cases (Figures 6-10). However, the exit is as good as the entrance. In part III of this series, I will do some of the clinical cases from a single crown to the dentistry of the complete quadrant that we have completed using our workflow and processes of dentistry of the day.

Figure This patient presented a decorated tooth, which required an emergency treatment on the same day.

Figure 7: CEER and the dentistry of the same day allow us to provide treatment modalities that were not otherwise possible in a single visit. Because the patient needed treatment the same day, we decided to keep the root. The post and the nucleus were carried out under the rubber dam.
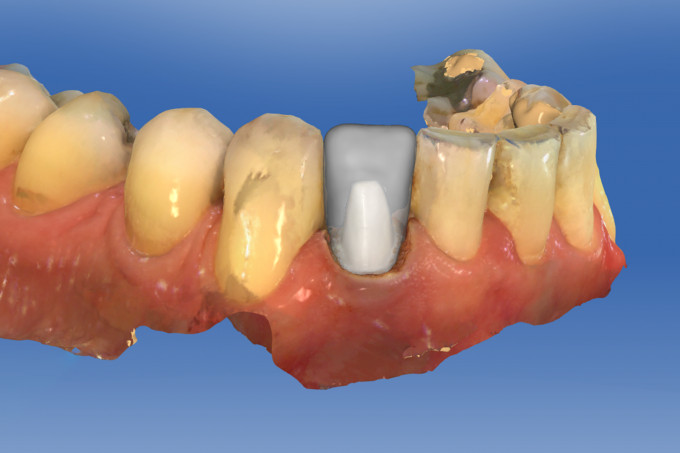
Figure 8: The preparation was scanned using Cerec Omnicam.

Figure 9: The final crown was designed presided using Cerec Omnicam.

Figure 10: The Final Crown of IPS EPS E.Max Cad Using CEREC MC XL achieved a great shadow game. This “temporary” solution otherwise has one leg in the patient’s mouth for 6 years and counting.